
Breast augmentation is one of the most commonly performed cosmetic surgeries in the United States. If you’re considering this procedure, you probably have questions about safety, costs, recovery, and results.
This guide covers everything you need to know, from choosing the right implants to understanding realistic recovery timelines. We’ve based this information on medical research, FDA data, and guidelines from board-certified plastic surgeons.
Table of Contents
What is Breast Augmentation?
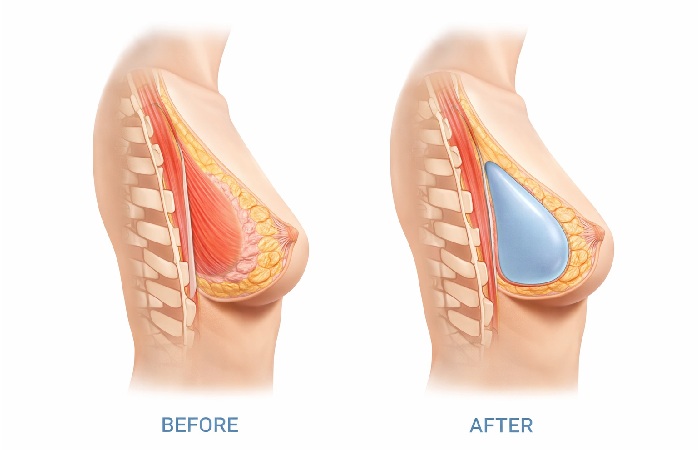
Breast augmentation, medically called augmentation mammaplasty, is a surgical procedure that increases breast size using implants or fat transfer. According to the American Society of Plastic Surgeons, more than 300,000 breast augmentation procedures were performed in 2023, making it one of the most popular cosmetic surgeries in the country.
The procedure involves placing implants under breast tissue or chest muscles to add volume and improve shape. It typically takes one to two hours and is performed under general anesthesia.
What Breast Augmentation Can Do
Breast augmentation is a cosmetic surgery that increases breast size and enhances shape using implants or fat transfer. Breast augmentation in Dallas is an example of this procedure, where saline or silicone implants are placed into the breast tissue to achieve fuller, more balanced breasts.
What Breast Augmentation Cannot Do
This procedure won’t fix significant sagging. If your nipples point downward or sit below your breast fold, you likely need a breast lift instead of or in addition to augmentation.
It also won’t guarantee perfect symmetry—most people have naturally asymmetric breasts, and surgery can improve but not eliminate this.
Who is a Good Candidate for Breast Augmentation?
The FDA approves breast implants for people who are at least 18 years old for saline implants and 22 years old for silicone gel implants.
Beyond age requirements, good candidates are physically healthy, have realistic expectations, and are bothered by small breast size or asymmetry.
You should be in good overall health without conditions that impair healing or increase surgery risks. Smoking significantly increases complications, so surgeons typically require you to quit at least several weeks before surgery.
You may not be a good candidate if you have active breast cancer or untreated precancerous breast lesions, are currently pregnant or breastfeeding, have uncontrolled diabetes or serious autoimmune conditions, or have unrealistic expectations about outcomes.
Some surgeons also recommend waiting if you’re planning pregnancy in the near future, as pregnancy and breastfeeding can change breast shape and potentially affect results.
Emotional Readiness and Expectations
Beyond medical factors, emotional readiness matters just as much. Breast augmentation is more likely to feel satisfying when you’re doing it for yourself—not to please a partner, friends, or social media.
Surgeons also watch for signs of body dysmorphic disorder or very unrealistic expectations. If you struggle with severe body image concerns, depression, or anxiety, it’s important to discuss this honestly with your surgeon and, if needed, a mental health professional before surgery.
A good consultation should feel like shared decision-making. That means your surgeon explains options, risks, and likely outcomes clearly, and you both decide together whether surgery fits your goals and lifestyle.
Medical Disqualifications
You may not be a good candidate if you have active breast cancer or untreated precancerous breast lesions, are currently pregnant or breastfeeding, have uncontrolled diabetes or autoimmune conditions, or have unrealistic expectations about outcomes.
Some surgeons also recommend waiting if you’re planning pregnancy in the near future, as pregnancy and breastfeeding can change breast shape and potentially affect results.
| Good Candidate | Not a Good Candidate |
|---|---|
| 18+ (saline) or 22+ (silicone) | Under minimum age |
| Healthy non-smoker | Active smoker |
| Realistic expectations | Expects perfection |
| Stable weight | Planning major weight changes |
| Finished with childbearing (preferred) | Currently pregnant/breastfeeding |
| Bothered by small size | Happy with current size |
When You May Need to Wait or Avoid Surgery
Your surgeon may advise delaying or avoiding breast augmentation if your chronic health conditions are poorly controlled, you smoke and are unwilling to quit, or you have an active infection anywhere in your body.
Surgery may also be postponed if you have major untreated mental health or body‑image issues, or if your goals don’t match what your anatomy can safely achieve—for example, wanting very large implants on a very narrow chest.
Waiting until your health, expectations, and life circumstances are stable usually leads to safer surgery and better long‑term satisfaction.
Types of Breast Implants
Choosing the right implant involves decisions about fill material, shape, texture, and size. Each option has different benefits and considerations.
Saline vs. Silicone Implants

Saline implants are filled with sterile salt water. They’re inserted empty and filled during surgery, which means they can use smaller incisions.
If a saline implant ruptures, your body safely absorbs the saline and the deflation is usually obvious within a short time.
Silicone implants are pre-filled with silicone gel that feels more like natural breast tissue. Most people find them softer and more natural-feeling than saline.
Because silicone implant ruptures can be “silent,” the FDA recommends periodic imaging (such as MRI or ultrasound) to check for rupture in women with silicone gel implants.
| Feature | Saline Implants | Silicone Implants |
|---|---|---|
| Feel | Firmer, may ripple | Softer, more natural |
| FDA minimum age | 18 years old | 22 years old |
| Rupture detection | Immediately obvious | May need MRI to detect |
| Incision size | Smaller (filled after insertion) | Larger (pre-filled) |
| Average cost difference | Slightly less expensive | Slightly more expensive |
Implant Shapes: Round vs. Teardrop
Round implants are the most common choice. They provide more fullness in the upper breast and maintain their appearance even if they rotate.
Teardrop implants, also called anatomical or “gummy bear” implants, have more volume at the bottom to mimic a natural breast slope. They are made with highly cohesive silicone gel that helps them hold their shape.
If a teardrop implant rotates, it can create an unnatural appearance and may require corrective surgery.
Implant Texture: Smooth vs. Textured
Smooth implants have a softer feel and can move naturally with breast tissue. They’re the most commonly used type in the United States.
Textured implants were designed to reduce capsular contracture risk and prevent rotation in teardrop implants. However, textured implants have been linked to a rare cancer called breast implant-associated anaplastic large cell lymphoma (BIA-ALCL).
As of mid‑2024, updates summarizing FDA data report roughly 1,300+ global cases and over 60 deaths related to BIA‑ALCL, highlighting that the condition is rare but serious.
Because of this risk, many surgeons now prefer smooth implants unless there’s a specific reason to use textured devices.
Choosing Your Implant Size
Implant size is measured in cubic centimeters (cc), not cup sizes. Cup sizes vary between bra manufacturers, but cc volume is consistent. Most breast augmentations use implants between 300cc and 500cc.
Your surgeon will help you choose based on your body frame, existing breast tissue, and desired outcome. Many surgeons use sizers during your consultation—you wear them in a sports bra under your clothes to see how different sizes look.
How Surgeons Help Choose Size and Shape?
Surgeons don’t just pick a cup size—they match implant width and projection to your chest width, skin stretch, and existing breast tissue. This helps avoid implants that are too wide or too narrow for your frame.
Many practices use in‑office sizers, 3D imaging, or photo galleries of patients with similar body types so you can see how different volumes and shapes might look on you. These tools reduce guesswork and help you feel more confident in your final choice.
The “Rice Test” for Sizing
Some surgeons recommend the rice test at home. Fill knee-high stockings with measured amounts of rice (300cc, 400cc, etc.) and place them in a non-padded bra. This gives you a rough idea of how different volumes look under clothing.
Remember that implants add volume behind your existing breast tissue, so the final result will look different than sizers worn in a bra. Photos of patients with similar builds to yours are often the most helpful sizing tool.
Popular Size Ranges
Based on plastic surgery data, here are typical implant sizes by body type:
- Petite frame (under 5’3″, 100-130 lbs): 250-350cc
- Average frame (5’3″-5’7″, 130-160 lbs): 350-450cc
- Athletic/larger frame (over 5’7″, 160+ lbs): 400-550cc
These are general guidelines only. Your chest width, existing breast tissue, and personal preference matter more than body weight alone.
Implant Placement Options
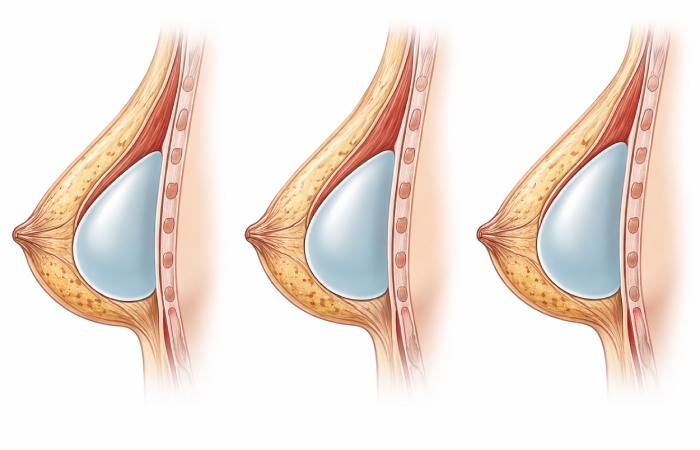
Where your surgeon places the implant affects recovery time, appearance, and long-term risks.
| Placement | Recovery Time | Look/Feel | Rippling Risk | Best For |
|---|---|---|---|---|
| Submuscular (under the muscle) | 2–3 weeks | Very natural | Low | Thin tissue, active lifestyle |
| Subglandular (over the muscle) | 1–2 weeks | More fullness on top | Higher | Adequate natural breast tissue |
| Dual plane (partial under muscle) | ~2 weeks | Natural look with good projection | Low | Most average patients |
Submuscular (Under the Muscle)
Submuscular placement puts the implant under your pectoralis major muscle. This provides more tissue coverage over the implant, which typically creates a more natural appearance, especially if you have minimal breast tissue.
Benefits include easier mammogram readings, lower rippling risk, and potentially lower capsular contracture rates. The main downside is a longer, more uncomfortable recovery period because the muscle must stretch to accommodate the implant.
Subglandular (Over the Muscle)
Subglandular placement puts the implant behind your breast tissue but in front of the chest muscle. This creates a shorter, less painful recovery and may provide more cleavage.
However, this placement has a higher risk of visible rippling, especially if you have thin breast tissue. Mammograms can also be slightly more difficult.
Dual Plane (Partial Submuscular)
Dual plane is a hybrid approach where the implant’s upper portion sits under the muscle while the lower portion sits under breast tissue only. This combines benefits of both placements—natural upper breast appearance with better lower breast projection.
| Placement | Recovery Time | Natural Appearance | Rippling Risk | Best For |
|---|---|---|---|---|
| Submuscular | 2-3 weeks | Very natural | Low | Thin tissue, active lifestyle |
| Subglandular | 1-2 weeks | More fullness on top | Higher | Adequate breast tissue |
| Dual Plane | 2 weeks | Natural + projection | Low | Most patients |
Incision Options
Your surgeon can access the breast pocket through several incision locations. Each has advantages regarding scarring and surgical precision.
- Inframammary (under breast fold): This is the most common approach. The incision sits in the natural fold under your breast, making it well-hidden. It provides excellent visibility during surgery and allows precise implant placement.
- Periareolar (around nipple): This incision follows your areola’s edge. Scars blend into the color transition between areola and skin. However, this approach has a slightly higher risk of decreased nipple sensation and may interfere with breastfeeding.
- Transaxillary (armpit): The incision is made in your armpit crease, leaving no scars on the breast itself. This approach requires an endoscope and offers less precision than other methods.
- Transumbilical (belly button): This rare approach uses an incision at your belly button. It only works with saline implants and offers the least surgical precision. Few surgeons perform this technique.
Most surgeons prefer the inframammary approach because it provides the best access and control during surgery while producing well-hidden scars.
Pre‑Surgery Evaluation and Preparation
Before surgery, your surgeon will review your medical history, examine your breasts, and sometimes recommend tests such as blood work or, in some cases, a baseline mammogram based on your age and risk factors.
You’ll usually be asked to stop smoking, avoid certain medications and supplements that increase bleeding (like some pain relievers or herbal products), and arrange for someone to drive you home and stay with you after surgery.
It also helps to set up your recovery space in advance. Keep essentials like medications, water, snacks, phone charger, and pillows within easy reach so you’re not stretching or lifting more than you should in the first few days.
The Breast Augmentation Procedure: Step-by-Step

Understanding what happens during surgery can help ease anxiety. Here’s the typical process:
Before Surgery
You’ll receive instructions to stop eating and drinking at midnight the night before. Certain medications, particularly aspirin and anti-inflammatory drugs, must be stopped one to two weeks before surgery because they increase bleeding risk.
Arrive at the surgical center in comfortable, loose-fitting clothing that buttons or zips in front. You won’t be able to lift your arms overhead easily after surgery.
During Surgery
Most breast augmentations take one to two hours. You’ll receive general anesthesia, meaning you’ll be completely asleep. Some surgeons offer twilight sedation for certain cases, but general anesthesia is more common.
Your surgeon makes the chosen incision, creates a pocket for the implant (either under muscle or breast tissue), inserts and positions the implant, then closes the incisions with layered sutures. Surgical drains are rarely needed for breast augmentation.
Immediately After Surgery
You’ll wake up in a recovery room wearing a surgical bra or compression garment. Most people feel groggy, sore, and tight in the chest. This is normal. You’ll need someone to drive you home and stay with you for at least the first 24 hours.
Recovery Timeline: What to Expect Week by Week

Recovery varies by individual, but here’s what most people experience:
Week 1: Immediate Recovery
Pain peaks in the first 48-72 hours. Most people describe it as tightness, soreness, or feeling like you did 1,000 push-ups. Prescription pain medication helps during this time.
Your breasts will be swollen, bruised, and sit high on your chest. This is temporary—implants “drop and fluff” over several weeks as swelling decreases and muscles relax.
Activity restrictions: No lifting anything over 5-10 pounds. No raising your arms above shoulder height. Sleep on your back with your upper body elevated. Most people take one week off work for desk jobs.
Weeks 2-4: Gradual Healing
Pain should significantly improve by week two. Many people switch to over-the-counter pain relievers or stop pain medication entirely.
Swelling continues decreasing. You can usually shower normally once your surgeon approves (typically 48 hours after surgery). You’ll have a follow-up appointment to check incision healing.
Activity restrictions: You can do light walking and gentle movement. No heavy lifting or vigorous exercise. Continue wearing your surgical bra or a supportive sports bra.
Months 2-3: Implants Settling
This is the “drop and fluff” phase. Your implants gradually settle into a more natural position. Swelling continues decreasing, and your breast shape becomes more defined.
Most people return to normal exercise at six to eight weeks, once their surgeon approves. Start with light cardio and gradually increase intensity.
Activity milestones: Most people can return to full exercise, including upper body workouts, by three months. High-impact activities may take longer.
Long-term Recovery (3-6 months)
Final results typically appear around six months. Your incision scars fade from red to pink to white over 12-18 months. Silicone scar sheets or gels can help minimize scarring.
Your implants should feel like a natural part of your body by six months. Initially firm breasts soften as your tissues adapt.
| Timeline | Pain Level | Swelling | Activity Level | Work Return |
|---|---|---|---|---|
| Days 1-3 | High (7-9/10) | Severe | Bed rest | No |
| Week 1 | Moderate (4-6/10) | High | Light activity | Desk job possible |
| Weeks 2-4 | Mild (2-4/10) | Moderate | Walking, daily tasks | Yes (most jobs) |
| Months 2-3 | Minimal (0-2/10) | Mild | Exercise returning | Full activity |
| Month 6+ | None | Resolved | Unrestricted | Full normal |
Post-Operative Care & What to Wear
Following post-op instructions carefully reduces complications and improves results.
Bra Requirements
You’ll wear a surgical bra or compression garment continuously for the first two to four weeks. This supports your breasts and helps control swelling. Your surgeon will tell you when you can switch to a regular sports bra.
Avoid underwire bras for at least six to eight weeks. Underwires can irritate incisions and interfere with healing. Once cleared, you can gradually introduce underwire bras.
Sleep Position
Sleep on your back with your upper body elevated at 30-45 degrees for at least two weeks. This reduces swelling and prevents pressure on incisions. Use pillows to prop yourself up, or sleep in a recliner if you have one.
Most surgeons allow side sleeping after four to six weeks and stomach sleeping after eight to twelve weeks.
Scar Care
Once incisions are fully closed (usually two weeks), you can begin scar massage. Gently massage scars with vitamin E oil or silicone scar gel in circular motions for five minutes, twice daily. This helps soften and flatten scars.
Protect scars from sun exposure for at least one year. UV exposure can darken scars permanently. Use sunscreen or keep scars covered when outdoors.
Warning Signs to Watch For
Contact your surgeon immediately if you experience fever over 101°F, increasing pain after initial improvement, foul-smelling discharge from incisions, or significant asymmetry that develops suddenly. These could indicate infection or other complications requiring medical attention.
Results: What Your Breasts Will Look Like
Setting realistic expectations helps ensure satisfaction with your results.
Initial Appearance
Immediately after surgery, your breasts will look swollen, sit high on your chest, and appear unnaturally round. This is temporary. As swelling decreases and muscles relax, implants drop into a more natural position over six to twelve weeks.
One breast may drop faster than the other, causing temporary asymmetry. This usually resolves on its own.
Final Results
At six months, you’ll see your true results. Your breasts should feel soft and move naturally. The degree of naturalness depends on your implant choice, placement, and existing breast tissue.
Larger implants tend to look less natural, especially on petite frames. Submuscular placement typically looks more natural than subglandular placement.
Cleavage Considerations
How much cleavage you get depends on your chest anatomy, not just implant size. If your breasts naturally sit wide apart on your chest, implants won’t create significant cleavage. Submuscular placement also creates less cleavage than subglandular placement because muscle keeps implants slightly separated.
Push-up bras can still enhance cleavage after augmentation, just as they did before surgery.
Long-term Changes
Your breast size and shape will change over time due to aging, weight fluctuations, and gravity. Implants themselves don’t sag, but the surrounding breast tissue does. Maintaining a stable weight helps preserve results longer.
Pregnancy and breastfeeding can also change breast appearance. Some people choose revision surgery after having children.
Risks and Complications
Like any surgery, breast augmentation carries risks. Understanding these helps you make an informed decision.
Common Side Effects
Nearly everyone experiences temporary swelling, bruising, and soreness. These resolve within weeks. Many people also have temporary nipple sensitivity changes—either increased sensitivity or numbness. Sensation typically returns to normal within a few months, though permanent changes occur in approximately 15% of patients.
Serious Complications
- Capsular contracture is the most common serious complication, occurring in approximately 10-20% of patients according to research published in medical journals. Your body naturally forms a capsule of scar tissue around any implant. If this capsule tightens and squeezes the implant, it can cause firmness, distortion, or pain. Severe cases require surgery to release or remove the capsule.
- Implant rupture can occur from trauma, compression during mammography, or spontaneous deflation. Saline implant ruptures are immediately obvious—the breast deflates within hours. Silicone ruptures may be “silent” and only detectable through MRI screening.
- Infection occurs in less than 2% of cases but can be serious. Most infections develop within the first few weeks after surgery. Treatment usually involves antibiotics, but severe infections may require temporary implant removal.
- Bottoming out happens when the implant drops below the natural breast fold, creating an empty upper breast and overly full lower breast. This requires surgical correction.
- Breast implant illness (BII) is a term some people use to describe symptoms they believe are related to their implants, including fatigue, joint pain, and cognitive issues. Large studies, including research published by the National Institutes of Health, have shown mixed results, and there is still no single proven cause, but some people do report symptom improvement after implant removal.
Talking to Your Surgeon About Breast Implant Illness
-
If you’re worried your implants might be affecting your health, your concerns should be taken seriously. A good surgeon will listen, ask about your symptoms, and explain what tests or next steps make sense for you.
-
Keep simple notes about when your symptoms started, how often they happen, and what makes them better or worse. This can help your surgeon decide on blood tests, scans, referrals, or whether to talk about implant removal as an option.
-
Even though research on BII is still ongoing, you should feel heard and supported and be given a clear follow‑up plan—not made to feel like you’re imagining things.
BIA-ALCL (Breast Implant-Associated Anaplastic Large Cell Lymphoma) is a rare type of lymphoma that can develop in the scar tissue around textured breast implants. As of 2024, the FDA has confirmed approximately 1,000 cases worldwide and 60 deaths. The condition is extremely rare but serious. Because of this risk, many surgeons now use smooth implants instead of textured.
| Complication | Frequency | Treatment Required |
|---|---|---|
| Swelling/bruising | Nearly 100% | None (resolves naturally) |
| Temporary sensation changes | 60-70% | None (usually resolves) |
| Capsular contracture | 10-20% | Possible revision surgery |
| Permanent sensation changes | ~15% | None available |
| Implant rupture (10-year rate) | 10-15% | Implant replacement |
| Infection | <2% | Antibiotics ± removal |
| BIA-ALCL (textured implants) | Very rare | Implant removal + treatment |
Breast Augmentation vs. Breast Lift: Which Do You Need?
Many people confuse these procedures, but they address different concerns.
Cosmetic Augmentation vs. Reconstruction
Cosmetic breast augmentation is done to enhance the size and shape of naturally developed breasts. Breast reconstruction with implants is different—it rebuilds the breast after mastectomy or major breast surgery.
Reconstruction often involves additional steps such as tissue expanders and staged procedures, and it is usually covered by health insurance under specific laws, unlike most cosmetic augmentation.
Breast Augmentation
Breast augmentation adds volume using implants or fat transfer. It’s best for people who want larger breasts but have minimal sagging. Augmentation doesn’t lift the nipple position or remove excess skin.
If your nipples point forward and sit above your breast fold, augmentation alone will likely give you the results you want.
Breast Lift (Mastopexy)
A breast lift repositions your nipples and reshapes breast tissue by removing excess skin. It doesn’t add volume—in fact, your breasts may appear slightly smaller after surgery due to tissue tightening.
If your nipples point downward or sit below your breast fold, you need a lift. The “pencil test” can help—if you can hold a pencil under your breast without it falling, you have some degree of sagging.
Combined Procedure
If you want larger breasts AND have significant sagging, you may need both procedures. This can be done simultaneously or staged (lift first, augmentation later).
Combined surgery means one recovery period but a longer, more complex operation. Discuss the risks and benefits with your surgeon.
| Procedure | Adds Volume | Lifts Position | Removes Skin | Scars | Recovery |
|---|---|---|---|---|---|
| Augmentation | Yes | No | No | Minimal | 2-4 weeks |
| Lift | No | Yes | Yes | Extensive | 3-6 weeks |
| Combined | Yes | Yes | Yes | Extensive | 4-6 weeks |
Non-Surgical Alternatives
If you’re not ready for implants, some alternatives exist, though results are limited.
Fat Transfer Breast Augmentation
Fat transfer, also called autologous fat grafting, removes fat from one body area via liposuction and injects it into your breasts. This is the only non-implant surgical option that actually increases breast size.
Results are subtle—typically one cup size maximum. You need enough body fat for harvesting, and approximately 30-40% of transferred fat is reabsorbed by your body. Multiple sessions may be needed for desired results.
Benefits include a very natural look and feel, no foreign material in your body, and body contouring at the liposuction site. Downsides include limited size increase, unpredictable reabsorption rates, and higher cost per unit of volume added compared to implants.
Types of Breast Augmentation and Alternatives
You can think about breast enhancement in three main groups: standard implant surgery, surgery without implants, and non‑surgical options with limited effect.
-
Breast implants (saline or silicone): The most common option, using implants placed under or over the muscle through different incision sites.
-
Hybrid augmentation (implant + fat): In some practices, surgeons combine a smaller implant with fat grafting around it for softer edges and a more natural contour.
-
Fat transfer only: Uses your own fat (taken with liposuction) to give a subtle, usually one‑cup‑size increase and improve shape without an implant.
-
External expansion devices: Vacuum/expander devices can cause mild tissue expansion with very consistent use over months, but changes are usually modest.
-
Skin‑tightening and “non-surgical lift” treatments: Lasers, radiofrequency, or threads may slightly tighten the skin but don’t truly increase breast volume.
-
Exercise and posture: Strengthening chest and back muscles can make your chest look better supported, but it doesn’t increase actual breast tissue.
What Doesn’t Work
- Breast enhancement pills and creams are widely marketed but don’t work. No oral supplement or topical cream has been proven to increase breast size in scientific studies. Save your money.
- Exercises can strengthen chest muscles, which may slightly improve breast shape and posture, but they don’t increase actual breast tissue size.
Breast Augmentation Cost
Breast augmentation is typically not covered by insurance because it’s considered cosmetic. You’ll pay out-of-pocket unless the procedure is reconstructive (for example, after mastectomy).
Average Cost Breakdown
According to American Society of Plastic Surgeons 2023 statistics, the average surgeon’s fee for breast augmentation is approximately $4,500. However, this is just one component of the total cost.
Total typical costs range from $5,000 to $10,000 depending on location, surgeon experience, implant choice, and surgical facility. Urban areas and coastal cities tend to be more expensive.
| Cost Component | Typical Range |
|---|---|
| Surgeon’s fee | $3,500–$6,000 |
| Anesthesia | $1,000–$1,500 |
| Surgical facility | $800–$1,500 |
| Implants | $1,000–$2,000 |
| Pre-op testing | $200–$500 |
| Post-op garments | $50–$150 |
| Follow-up visits | Usually included |
| Total | $5,000–$10,000 |
Geographic Variations
Costs vary significantly by location. Major metropolitan areas like New York, Los Angeles, and San Francisco typically charge 20–40% more than smaller cities or rural areas. However, traveling far for surgery isn’t always recommended—you need local access to your surgeon for follow-up appointments and any complications.
Financing Options
Many plastic surgery practices offer financing through companies like CareCredit or Alphaeon. These medical credit cards provide payment plans, often with promotional interest-free periods.
Some surgeons also offer in-house payment plans. Always read the fine print regarding interest rates, fees, and what happens if you miss a payment.
Insurance Coverage
Insurance typically doesn’t cover cosmetic breast augmentation. However, reconstructive breast surgery after mastectomy is covered under the Women’s Health and Cancer Rights Act of 1998, which requires insurance plans that cover mastectomy to also cover reconstruction.
If you have tuberous breast deformity or severe asymmetry, insurance may cover surgery in some cases, but detailed documentation and pre-authorization are essential.
Typical Cost by Country
Costs vary widely between countries. The ranges below are approximate package prices that often include the surgeon’s fee, anesthesia, facility, and implants, but details depend on the clinic and city.
| Country | Typical Total Cost (approx.) | Notes |
|---|---|---|
| United States | $5,000 – $10,000 | Higher fees for surgeon, facility, and implants; major cities often at the top of the range. |
| Canada | $6,000 – $8,000 | Prices vary by province and clinic; often similar to or slightly below large U.S. metro areas. |
| United Kingdom | £3,500 – £7,000 | Private clinics set their own fees; London tends to be more expensive than regional centers. |
| Australia | AUD 10,000 – 15,000 | Often includes surgery, anesthesia, and hospital costs; big-city clinics sit at the higher end. |
| India | $3,000 – $4,500 | Typically lower labour and facility costs; popular for medical tourism but surgeon and hospital quality vary. |
| Mexico | $3,500 – $4,500 | Frequently marketed to medical tourists; total price may include travel-support packages. |
| Turkey | $3,000 – $5,000 | Known as a lower-cost hub for cosmetic surgery with package deals that may include hotel and transfers. |
| Brazil | $3,800 – $6,000 | Large cosmetic surgery market with many high-volume surgeons in major cities. |
Lower prices abroad can be attractive, but it’s important to check the surgeon’s credentials, facility accreditation, infection control standards, and what aftercare is realistically available once you return home.
Special Considerations
Several important topics deserve extra attention if you’re considering breast augmentation.
Most people can breastfeed successfully after breast augmentation, and implant surgery does not automatically prevent milk production. However, some factors can make breastfeeding more difficult, such as periareolar incisions that may affect milk ducts and nerves, pre‑existing breastfeeding problems, or very limited natural breast tissue.
If future breastfeeding is important to you, tell your surgeon during your consultation. In many cases, an inframammary (breast fold) incision is preferred because it has the lowest chance of interfering with breastfeeding.
You can and should continue getting mammograms after breast augmentation. Implants do not increase breast cancer risk, but they can make images harder to interpret, which is why you must always tell the technician you have implants. They can then use implant displacement views, which gently move the implant back against the chest wall so more breast tissue can be seen.
The FDA recommends periodic imaging such as MRI or ultrasound for people with silicone implants to check for silent ruptures, although not all insurance plans cover this. Submuscular placement generally makes mammogram interpretation easier than subglandular placement because more breast tissue sits in front of the implant.
Implant Lifespan and Replacement

Breast implants are not lifetime devices. They don’t have a fixed expiration date, but the longer you have them, the more likely you are to develop issues such as rupture, capsular contracture, or changes in position that may require surgery.
According to FDA guidance, many surgeons suggest thinking about the possibility of replacement somewhere in the 10–20‑year range, but if your implants look and feel normal and you have no symptoms, routine replacement isn’t automatically required.
Common reasons for revision surgery include implant rupture or deflation, capsular contracture causing firmness or distortion, a desired size change, implant shifting or “bottoming out,” and normal aging changes in breast shape. Around 1 in 5 augmentation patients will need some form of additional breast or implant surgery within about 10 years.
Long‑Term Follow-Up and Monitoring
Breast implants require long‑term follow-up, even when you feel fine. Most surgeons recommend periodic visits to check breast shape, firmness, and any new symptoms over the years.
For silicone gel implants, your surgeon may suggest MRI or ultrasound at intervals, especially if you notice changes in how your breasts look or feel.
Contact your surgeon promptly if you notice sudden swelling, a new lump, marked asymmetry, persistent pain, or fluid around the implant area. These signs don’t always mean a serious problem, but they should be evaluated quickly to rule out complications.
How to Choose a Qualified Plastic Surgeon
Your surgeon choice is the single most important factor affecting your safety and results.
Board Certification
Choose a surgeon certified by the American Board of Plastic Surgery (ABPS). This is the only board recognized by the American Board of Medical Specialties for plastic surgery. Board certification requires:
- Completion of plastic surgery residency training (typically 6-7 years after medical school)
- Passage of comprehensive written and oral examinations
- Ongoing continuing medical education
Some doctors claim to be “board certified” in cosmetic surgery by lesser-known boards that don’t require the same rigorous training. Always verify ABPS certification at the American Board of Medical Specialties website.
Experience and Specialization
Ask how many breast augmentations your surgeon performs annually. Surgeons who regularly perform a procedure tend to have better outcomes and lower complication rates. Look for someone who performs at least 50-100 breast augmentations per year.
Review before-and-after photos of the surgeon’s actual patients, particularly those with builds similar to yours. Be wary of stock photos or photos that look too perfect—they may not be real patient results.
Hospital Privileges
Make sure your surgeon has admitting privileges at a nearby hospital. This indicates the hospital has vetted their credentials and skills. If a complication occurs, you want your surgeon able to provide hospital care if needed.
Red Flags to Avoid
Be cautious if a surgeon:
- Isn’t board certified by ABPS
- Pressures you to book surgery during the first consultation
- Offers prices significantly below the market average
- Guarantees perfect results
- Dismisses your concerns or questions
- Doesn’t require a physical examination before providing recommendations
- Performs surgery in an unlicensed facility
Questions to Ask at Your Consultation
Come prepared with questions:
- Are you board certified by the American Board of Plastic Surgery?
- How many breast augmentations do you perform each year?
- What’s your complication rate for this procedure?
- What’s your revision rate (percentage of patients needing additional surgery)?
- What size and type of implant do you recommend for my goals and body type?
- What placement and incision approach do you suggest, and why?
- May I see before-and-after photos of patients with similar builds?
- What happens if I need revision surgery—what are the costs?
- Where will you perform my surgery? Is it an accredited facility?
- Who will administer anesthesia? What are their credentials?
A qualified surgeon will answer these questions thoroughly and make you feel comfortable.
Frequently Asked Questions
1. Am I a good candidate for breast augmentation?
You may be a good candidate if you’re healthy, at least 18 for saline or 22 for silicone, a non‑smoker or willing to quit, and bothered by small or uneven breasts. Your surgeon will also review your medical history, breast anatomy, and expectations before recommending surgery.
2. How long is breast augmentation recovery and when can I go back to work?
Most people feel the worst discomfort in the first 2–3 days and then improve over the first week. Many return to desk jobs in about a week, but heavy lifting and intense workouts are usually restricted for 4–6 weeks, depending on your surgeon’s advice.
3. Will breast implants affect my ability to breastfeed?
Many people breastfeed normally after augmentation. However, periareolar incisions and pre‑existing breastfeeding problems can make it harder, so if breastfeeding is important to you, tell your surgeon so they can choose the safest incision and technique.
4. Will breast implants interfere with mammograms or cancer screening?
You can still have regular mammograms with implants. Always tell the imaging center you have implants so they can use special implant displacement views to see more tissue. Implants don’t increase breast cancer risk but do require extra care in imaging.
5. Do breast implants need to be replaced every 10 years?
There is no strict 10‑year rule. Implants are not lifetime devices, and many people eventually need another surgery for rupture, capsular contracture, or shape changes, but if your implants look and feel fine and you have no issues, routine replacement at exactly 10 years isn’t mandatory.
6. What is the difference between implants under vs over the muscle?
Under‑the‑muscle placement usually looks more natural and may make imaging easier but can mean more soreness early on. Over‑the‑muscle placement often has a quicker recovery and more upper‑pole fullness but can show more rippling in people with thinner tissue.
7. How much does breast augmentation cost?
In the US, most people pay somewhere between $5,000 and $10,000 including surgeon, facility, anesthesia, and implants. Costs vary by city, surgeon experience, implant choice, and whether you’re having surgery at a hospital or a private surgical center.
You can replace your current FAQ block with just these 7 and you’re still well‑aligned with search + voice intent.
Final Thoughts
Breast augmentation can significantly improve your confidence and satisfaction with your appearance when performed for the right reasons with realistic expectations. The key to a positive outcome is choosing a qualified surgeon, understanding the procedure thoroughly, and being honest with yourself about your motivations and expectations.
Take your time making this decision. Consult with multiple board-certified plastic surgeons, review their work, and ensure you feel comfortable with your choice. A good surgeon will answer all your questions, never pressure you, and prioritize your safety above all else.
Remember that while complications are relatively uncommon, they do occur. Understanding the risks helps you make an informed decision and recognize when something needs medical attention.
If you decide breast augmentation is right for you, following your surgeon’s pre-op and post-op instructions carefully will give you the best chance of a smooth recovery and beautiful results.