
Facing breast reconstruction after mastectomy is deeply personal—and often overwhelming. If you’re researching implant-based options, you likely want straightforward answers: What actually happens during this surgery? What will recovery feel like? Could this be right for me? This guide cuts through medical jargon to explain implant-based breast reconstruction in plain language, covering how it works, key risks to understand, and practical steps to prepare for a confident conversation with your surgical team. Important: This information is for educational purposes only and does not replace personalized medical advice from a board-certified plastic surgeon.
Table of Contents
Summary
- What it is: Surgery using silicone or saline implants to restore breast shape after mastectomy.
- Two main approaches: Two-stage (tissue expander first) or direct-to-implant (single surgery).
- Key decision point: Prepectoral (over muscle) vs. subpectoral (under muscle) placement affects recovery and aesthetics.
- Critical consideration: Prior or planned radiation therapy significantly increases complication risks—discuss timing carefully with your team.
- Next step: Prepare 3–5 specific questions for your surgeon consultation using our checklist below.
- This is one option; flap reconstruction and choosing to go flat are valid alternatives that your team can help you compare.
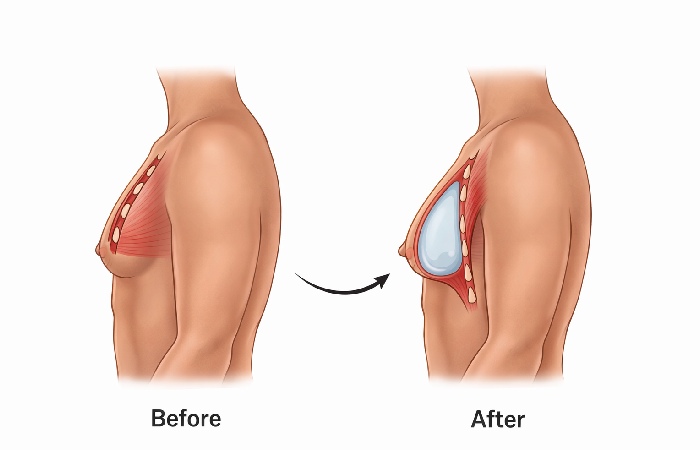
What Is Implant-Based Breast Reconstruction?
Implant-based breast reconstruction is surgery that restores breast shape using a silicone or saline implant after mastectomy. Unlike flap reconstruction (which uses your own tissue), this approach places a medical-grade implant to recreate volume and contour. The procedure is typically performed by a board-certified plastic surgeon, often in coordination with your breast cancer surgical team. While it cannot replicate the exact sensation or appearance of natural breast tissue, many patients report improved body confidence and comfort in clothing after healing, as described in the Mayo Clinic’s overview of breast reconstruction.
It is one of several reconstruction options. Some patients choose autologous (flap) reconstruction using their own tissue, and others choose no reconstruction (“going flat”). Your team can help you compare these paths based on your health, anatomy, and treatment plan.
How the Procedure Works: Two Main Pathways
Most implant-based reconstructions follow one of two pathways. Understanding the difference helps set realistic expectations.
Two-Stage Reconstruction with Tissue Expander
This remains the most common approach, especially when skin preservation is limited or radiation is planned.
- Stage 1 (Mastectomy day or soon after): A temporary, balloon-like tissue expander is placed under the chest skin and muscle. A small valve remains under the skin for access.
- Expansion phase (weeks to months): In clinic visits, your care team gradually injects saline through the valve, slowly stretching the skin and muscle to create space for a permanent implant.
- Stage 2 (Exchange surgery): Once expansion is complete, a second surgery replaces the expander with a permanent silicone or saline implant.
Why choose this path? It allows careful adjustment of breast size and shape over time and is often preferred if postmastectomy radiation is needed, as expansion can pause during treatment, as outlined in the National Cancer Institute breast reconstruction fact sheet.
Direct-to-Implant (DTI) Reconstruction
In select cases, a permanent implant is placed immediately during mastectomy, skipping the expander phase.
- Best suited for: Patients with adequate skin preservation, no planned radiation, and favorable anatomy.
- Advantage: Fewer surgeries and a faster overall timeline.
- Trade-off: Less flexibility to adjust size and shape after initial placement; higher likelihood of revision if complications arise or cosmetic goals change.
In practice, surgeons often make a final decision about two-stage vs. DTI during surgery, based on how healthy and well-vascularized the mastectomy skin flaps appear.
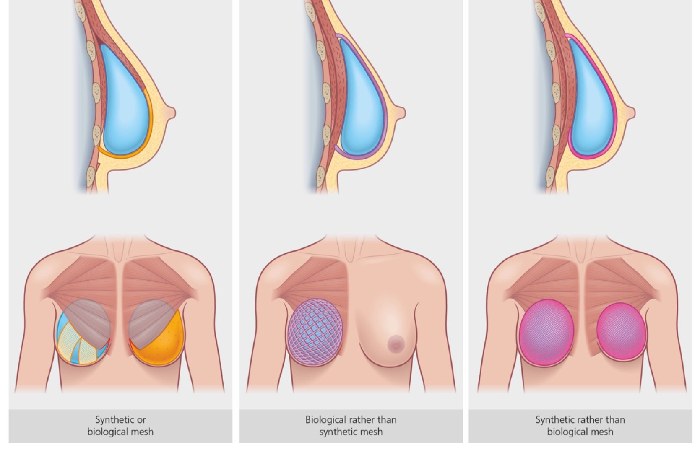
Implant Placement: Prepectoral vs. Subpectoral
Where the implant sits relative to your chest muscle significantly impacts recovery and long-term results.
Note: Surgeons may use acellular dermal matrix (ADM)—a biological or synthetic mesh—to support implant positioning and improve contour, especially in prepectoral cases. These materials act as an internal scaffold and can help define the breast fold and lower-pole shape.
Types of Implants: Silicone vs. Saline
Both options have a silicone outer shell; the difference is the filler.
Current practice note: Smooth, round silicone implants are most commonly used in the U.S. for reconstruction due to their safety profile and natural feel. Textured implants carry a small but real risk of breast implant-associated anaplastic large cell lymphoma (BIA‑ALCL) and are no longer considered first-line in most settings, as detailed on the FDA page on BIA‑ALCL.
Key Risks and Complications to Understand
All surgeries carry risks. Being informed helps you weigh benefits thoughtfully with your team. Your individual risk depends on factors like smoking status, diabetes or other health conditions, any prior or planned radiation, and your surgeon’s technique and experience.
Surgical Risks (Short-Term)
- Infection, bleeding, or slow wound healing (reported in a small but meaningful percentage of patients, and higher in smokers or those with other medical conditions).
- Reaction to anesthesia.
- Fluid buildup (seroma) requiring drainage.
- Skin or nipple healing problems if blood supply is compromised.
Implant-Specific Risks (Long-Term)
- Capsular contracture: Scar tissue tightens around the implant, causing firmness, distortion, or pain. It is graded on the Baker Scale (I–IV); grades III–IV may require revision surgery.
- Implant rupture or leakage: Silicone implants can rupture without obvious external change, which is why imaging surveillance is advised; saline ruptures are immediately visible because the implant deflates.
- Changes in sensation: Numbness or altered feeling in the breast/chest wall is common and may be long-lasting.
- Need for future surgery: Implants are not lifetime devices. Many patients need replacement or removal at some point due to complications, cosmetic changes, or normal aging of the body.
Critical Factor: Radiation Therapy
Postmastectomy radiation therapy (PMRT) significantly increases risks of problems such as infection, capsular contracture, and implant loss. These effects have been observed across multiple clinical studies and are especially important to consider for prepectoral reconstruction. If radiation is planned or likely, discuss timing strategies with your oncology and reconstruction teams. Some patients opt for delayed reconstruction, a staged expander approach, or flap-based options in this scenario.
Who Is a Good Candidate? Key Considerations
Implant-based reconstruction isn’t right for everyone. Factors your surgical team will evaluate:
✅ May be a good fit if you:
- Have adequate chest skin and tissue after mastectomy.
- Are not planning postmastectomy radiation (or have completed it with good healing and acceptable tissue quality).
- Maintain a stable, healthy weight.
- Do not smoke (or can quit well before surgery—smoking drastically increases complication risks; organizations like Macmillan Cancer Support stress this).
- Prefer shorter initial surgery and recovery compared with flap procedures.
❌ Proceed with caution or consider alternatives if you:
- Require or have recently completed radiation therapy to the chest wall.
- Have significant obesity or a very large natural breast on the other side, which can make symmetry more challenging.
- Are an active smoker (most surgeons require documented cessation before proceeding).
- Have uncontrolled medical conditions affecting healing (e.g., poorly controlled diabetes, vascular disease).
Remember: Candidacy is highly individual. A board-certified plastic surgeon will assess your anatomy, cancer treatment history, and personal goals to recommend the safest, most effective option for you, including whether flap reconstruction or going flat may better meet your priorities. You can learn more about these options in the American Society of Plastic Surgeons breast reconstruction information.
If you’re still deciding whether implants match your goals and medical situation, this guide to implant-based breast reconstruction offers additional context on candidacy and expectations.
What to Expect: Recovery Timeline Guide
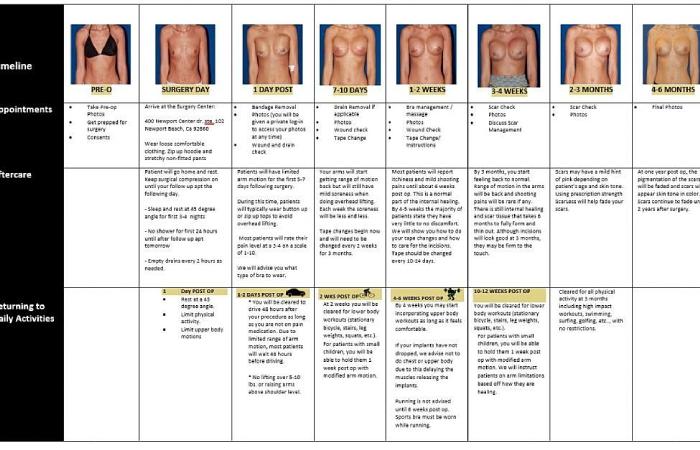
Recovery is gradual. Setting realistic expectations reduces anxiety.
Weeks 1–2: Initial Healing
- Hospital stay: Typically 1–2 days for expander placement; some direct-to-implant procedures may be done as outpatient or overnight stays, depending on your health and hospital protocol.
- Activity: Rest with arms at sides; avoid lifting more than about 5 lbs, overhead reaching, or driving until cleared.
- Pain management: Prescription medication initially, transitioning to over-the-counter options as you improve.
- Drain care: Temporary tubes may collect fluid; your team will instruct you on emptying and monitoring.
Weeks 3–6: Gradual Return to Activity
- Expansion visits begin (if two-stage): Weekly or biweekly saline injections to stretch tissue.
- Movement: Light walking is encouraged; avoid strenuous exercise, heavy lifting, or high-impact activity.
- Appearance: Swelling and bruising gradually improve; your final breast shape is not yet visible.
Months 2–6: Refinement and Final Steps
- For two-stage: Exchange surgery typically occurs 3–6 months after expansion completes (longer if radiation was given or if healing is delayed).
- Daily life: Most patients resume normal daily activities by about 6–8 weeks; full aesthetic settling may take 6–12 months.
- Nipple reconstruction: If desired, this is usually performed after implant healing is complete, followed by areola tattooing for color.
Tip: Keep a symptom journal and attend all follow-ups. Report sudden pain, redness, fever, or unusual swelling immediately.
Preparing for Your Surgeon Consultation: 5 Essential Questions
Come prepared to make the most of your consultation. These questions help clarify options and align expectations:
- “Given my cancer treatment history (especially radiation), which reconstruction approach do you recommend and why?”
- “What are your personal experience and outcomes with prepectoral vs. subpectoral placement?”
- “What is your protocol if capsular contracture or infection occurs?”
- “What does long-term implant surveillance involve for me, and who manages it?”
- “Can I see before-and-after photos of patients with anatomy and treatment plans similar to mine?”
Pro tip: Bring a trusted friend or family member to take notes. Record the conversation (with permission) if helpful.
Common Mistakes to Avoid
- Rushing the decision: Take time to understand options. Many centers offer second opinions, and waiting for clearer pathology or treatment plans is often appropriate.
- Overlooking surgeon credentials: Verify board certification in plastic surgery (not just “cosmetic surgery”) and hospital privileges; you can search via the American Board of Plastic Surgery.
- Underestimating recovery: Plan for 6–8 weeks of modified activity; arrange help at home, especially if you have young children or a physically demanding job.
- Ignoring long-term commitment: Implants require monitoring over many years. Factor in future imaging for silicone implants and potential revision surgeries.
- Comparing only to pre-cancer appearance: Focus on symmetry, comfort, and confidence in clothing—not perfectly replicating your exact prior breast.
Final Verdict: Is Implant-Based Reconstruction Right for You?
Implant-based breast reconstruction offers a well-established path to restore breast shape after mastectomy, with advantages of shorter initial surgery and no donor-site scarring compared to flap procedures. However, it involves trade-offs: potential for future surgeries, implant-specific risks, and sensitivity to radiation history. The strongest predictor of satisfaction is not the technique alone—it is clear communication with a skilled, board-certified surgical team who listens to your priorities. If you’re considering this option, prioritize consultations with surgeons who transparently discuss risks, show relevant outcome photos, and partner closely with your oncology team.
Frequently Asked Questions
Q: How long do breast implants last after reconstruction?
A: Implants aren’t lifetime devices. Many last 10–15+ years, but factors like radiation, aging, or complications may require earlier replacement. For silicone implants, the FDA recommends imaging (ultrasound or MRI) starting around 5–6 years after placement and every few years thereafter, according to the FDA screening recommendations for silicone breast implants. Regular follow-up with your surgeon is essential.
Q: Can I have implant reconstruction if I need radiation therapy?
A: Yes, but radiation increases risks of capsular contracture, healing problems, and implant loss. Your team may recommend delaying reconstruction, using a staged expander approach, choosing a subpectoral plane, or considering flap-based options. Timing discussions with both oncology and plastic surgery are critical.
Q: What is capsular contracture, and can it be prevented?
A: Capsular contracture is scar tissue tightening around the implant, potentially causing firmness or distortion. While it cannot be completely prevented, techniques such as careful surgical handling, minimizing infection risk, and selective use of mesh or ADM may help lower the chance. Treatment ranges from observation to revision surgery.
Q: Will I have feeling in my reconstructed breast?
A: Nipple and breast sensation is often reduced or altered after mastectomy and reconstruction. Some sensation may return over 1–2 years, but full restoration is uncommon. Ask your surgeon about nerve-sparing techniques or emerging nerve graft (“neurotization”) options if sensation is a priority at your center.
Q: How soon can I return to work or exercise?
A: Most patients resume desk work in about 2–4 weeks and light exercise around 6 weeks. Full activity, including heavy lifting or high-impact exercise, typically requires 8–12 weeks. Always follow your surgeon’s personalized guidance, which may differ based on your specific procedure and healing.
Q: Are there alternatives to implant-based reconstruction?
A: Yes. Flap reconstruction (using your own tissue from the abdomen, back, or thighs) offers a more natural feel and does not require implants, but involves longer surgery and donor-site recovery. Some patients also choose to go flat without reconstruction. Your surgeon can compare all options based on your anatomy, cancer plan, and goals.