
")
For 34 years, military families at Camp Lejeune drank, cooked with, and bathed in water laced with industrial solvents. Most never knew. By the time the contaminated wells were finally shut down in the mid-1980s, government estimates suggest as many as one million people — service members, spouses, children, and civilian workers — had been exposed to chemicals linked to cancer, organ damage, and neurological disorders.
This isn’t ancient history. Veterans are still getting diagnosed decades after leaving the base. Legal claims are still being filed under a law that didn’t exist until 2022. And the government is still figuring out how to process all of them.
Below is a simple, easy-to-understand outline: of what occurred, the realities of the science (and its limitations), how you can take advantage of this benefit, and how you can get the most from it, free of false claims or a sales pitch that much of Camp Lejeune material on the internet.
Table of Contents
Camp Lejeune’s Crisis at a Glance:
- What happened?→ Industrial solvents (TCE, PCE, benzene, vinyl chloride) added to water supplies at Camp Lejeune, NC during 1953-87 by off-base dry cleaner and on-base industrial activities.
- What health conditions are associated?-> 8 conditions are eligible for VA disability pay; 15 are eligible for VA healthcare with no copay including several types of cancer, Parkinson‘s disease, and kidney disease.
- Can affected people get benefits? → Yes — through VA disability claims (no lawyer needed) and/or the Camp Lejeune Justice Act of 2022 (federal lawsuit or Navy’s elective option).
- Does a lawsuit affect VA benefits? → Filing does not. But a court-awarded judgment may be reduced by prior VA payments related to Camp Lejeune exposure.
What Happened at Camp Lejeune? A 34-Year Timeline
Camp Lejeune‘s water crisis is the contamination of drinking water at Marine Corps Base Camp Lejeune in Jacksonville, North Carolina from 1953 through 1987. Several industrial solvents, most notably trichloroethylene (TCE) and perchloroethylene (PCE), leaked from an off-base dry cleaner and numerous on-base industrial plants into the base‘s water supply, possibly exposing as many as one million people to chemicals well in excess of federal drinking water limits.
That definition barely scratches the surface. Here’s how it unfolded.
The Contamination Sources (1953–1985)

Camp Lejeune, itself, had two water treatment systems Tarawa Terrace and Hadnot Point and each had its own contamination story. It is important to distinguish which is which, because the science, the data gaps, and the legal implications for each are different.
Tarawa Terrace served enlisted family housing. Its primary contaminant was PCE, which seeped into the groundwater from ABC One-Hour Cleaners, an off-base dry cleaning operation. Spills and improper disposal practices sent PCE migrating through the soil and into the wells that fed this system. According to a National Research Council report published through the National Institutes of Health, ATSDR modeling estimated that PCE concentrations in Tarawa Terrace’s finished water exceeded the EPA’s maximum contaminant level (MCL) of 5 μg/L from as early as November 1957 until the wells were closed in 1985.
Hadnot Point supplied water to barracks, administrative offices, the base hospital, and an industrial area. Its contamination was far more complex — multiple sources, multiple chemicals. TCE was the most prevalent contaminant. It was probably the result of spills at industrial sites, leaking underground storage tanks, drums at dump sites and a former fire training area. They also found the following chemicals: PCE; vinyl chloride; benzene; methylene chloride; toluene.
Put plainly: we still don’t have a complete picture of what happened at Hadnot Point. While ATSDR completed historical modeling for Tarawa Terrace, no equivalent modeling has been completed for Hadnot Point. The full extent of contamination there remains scientifically uncharacterized — which is a significant gap, given that Hadnot Point served the base hospital, barracks, and administrative buildings.
How the Crisis Was Discovered — and Why It Took So Long
It took until the early 1980s — roughly three decades into the contamination — for routine water testing to flag the problem. Once identified, contaminated wells were shut down between November 1984 and May 1985. The entire Tarawa Terrace treatment plant followed in 1987.
Yet, there is a long 34-year interval from the start of the source (1953) and the actual response (1984–1987). During that period, the water supply had turned on-and-off, during which time the level of substance in the water would come and go sometimes significantly based on which wells were turned on. The ingoing resident had no way of knowing if that sip was substantially contaminated or just okay.
Key Milestones
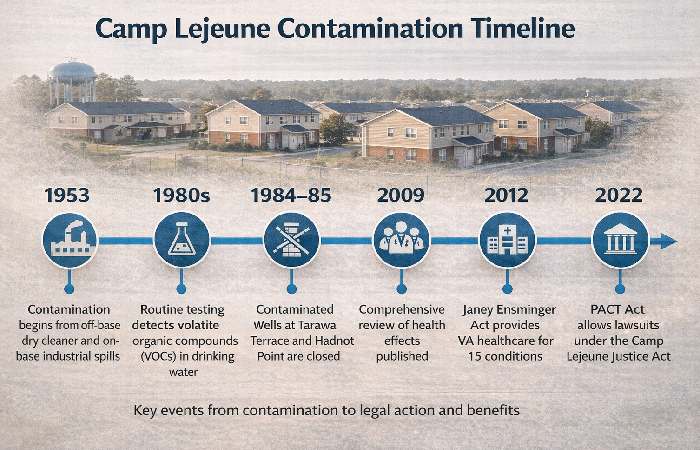
| Year | Event |
|---|---|
| 1953 | ABC One-Hour Cleaners begins operations near Tarawa Terrace wells |
| 1957 | ATSDR models estimate PCE first exceeded EPA limits in Tarawa Terrace water |
| 1980s | Routine testing reveals VOC contamination in multiple wells |
| 1984–85 | Contaminated wells at both systems are closed |
| 1987 | Tarawa Terrace water-treatment plant shut down entirely |
| 2009 | National Research Council publishes comprehensive health effects review |
| 2012 | Janey Ensminger Act provides VA healthcare for 15 covered conditions |
| 2017 | VA establishes 8 presumptive conditions for disability compensation |
| 2022 | PACT Act signed — includes Camp Lejeune Justice Act allowing lawsuits |
What Chemicals Contaminated the Water?
Four primary contaminants drove Camp Lejeune’s crisis. Each has a distinct toxicological profile.
TCE, PCE, Benzene, and Vinyl Chloride — Explained

Trichloroethylene (TCE) — An industrial degreasing solvent. TCE was the dominant contaminant at Hadnot Point. It is classified as a known human carcinogen by the EPA’s Integrated Risk Information System. Chronic exposure is associated with kidney cancer, liver damage, and neurological effects.
Perchloroethylene (PCE) — A dry-cleaning solvent. PCE was the primary contaminant at Tarawa Terrace, supplied by an on-base dry cleaner. PCE undergoes natural groundwater degradation into TCE, trans-1,2-dichloroethylene, and vinyl chloride–a single source producing many toxic compounds. EPA ranks PCE as a probable human carcinogen.
Benzene — A volatile organic compound found in fuels and industrial chemicals. Benzene is a known human carcinogen with strong associations with leukemia and blood disorders. It was detected in Hadnot Point supply wells.
Vinyl Chloride a breakdown product of TCE and PCE. Vinyl chloride is a human carcinogen which has been most frequently associated with liver (hepatic angiosarcoma) cancer. Vinyl chloride was found at Camp Lejeune as a secondary product of the original solvent/contaminant.
Tarawa Terrace vs. Hadnot Point: Two Contamination Scenarios
| Factor | Tarawa Terrace | Hadnot Point |
|---|---|---|
| Primary Contaminant | PCE | TCE |
| Source | Off-base dry cleaner (ABC One-Hour Cleaners) | Multiple on-base industrial sites, leaking tanks, dump sites |
| Population Served | Enlisted family housing | Barracks, admin offices, base hospital, industrial area |
| Contamination Complexity | Single primary source | Multiple sources, multiple chemicals |
| Historical Modeling Completed? | Yes (ATSDR) | No — not yet characterized |
| MCL Exceedance Duration | ~1957 to 1985 (estimated) | Unknown (insufficient data) |
| Other Chemicals Detected | TCE, vinyl chloride (degradation products) | PCE, vinyl chloride, benzene, methylene chloride, toluene |
However, it was not only drinking that caused the exposures. What made the contamination at Camp Lejeune so insidious were the volatile organic compounds (VOCs) substances at room temperature tend to evaporate so readily that when one is using the water at any moment, one is also inhaling and absorbing those compounds in the air. Both TCE and PCE are VOCs. In addition to drinking using the water to drink, cook, and wash one‘s hands people were absorbing them through bathing, showering, dishwashing, laundry, and swimming.
Health Effects Linked to Camp Lejeune’s Crisis
Here’s where most other sources either overstate the case or dodge it entirely. The reality sits in an uncomfortable middle ground — and understanding it honestly is more useful than false certainty in either direction.
How Strong Is the Evidence? Understanding the Science
Federal scientific review of the health impacts of Camp Lejeune is by a National Research Council committee report at the request of Congress. That committee used a 5-level classification system of strength of evidence. Only two were relevant for TCE and PCE:
- Limited/suggestive evidence of an association — Studies suggest a link, but chance and bias cannot be fully ruled out. Not sufficient to infer causation.
- Inadequate/insufficient evidence — Not enough data to determine whether an association exists.
Absolutely none of the health outcomes we looked at met the threshold for “sufficient evidence of a causal relationship”. I don‘t want to scare you (or the chemicals), but instead to let you know that the studies we have just weren‘t powerful enough: they involved small sample sizes, had imperfect estimates of chemical exposures and struggled to assess health outcomes in a highly mobile military population over a long period of time.
Here’s what the science does support, and to what degree.
Cancers Associated with TCE and PCE Exposure
The epidemiologic literature provides limited/suggestive evidence of associations between chronic TCE or PCE exposure and:
- Kidney cancer — The strongest concordance between human and animal data; kidney tumors observed in workers exposed to high levels of TCE
- Bladder cancer
- Breast cancer
- Esophageal cancer
- Lung cancer
Animal studies additionally showed liver cancer in mice and testicular cancer in male rats exposed to TCE, and mononuclear-cell leukemia in rats exposed to PCE. However, many of these tumors were species-, gender-, and strain-specific — meaning direct extrapolation to humans requires caution.
Non-Cancer Health Conditions
Beyond cancer, the research identified several other health concerns:
- Hepatic steatosis (fatty liver disease) Limited/suggestive evidence at high exposure levels
- Renal toxicity (kidney damage) – Inadequate/ suggestive evidence at high chronic exposure
- Neurobehavioral effects Limited/suggestive evidence for visuomotor deficits, fatigue, headache, concentration impairment; most effects found during active exposure, limited data on persistence.
- Scleroderma Limited for SSc or supportsiveness, especially if exposed to TCE
- Male infertility — Some evidence from animal studies; human data inconsistent
- Miscarriage — Epidemiologic evidence suggests increased risk during (not before) pregnancy exposure
- Immune system effects — TCE acts as a skin sensitizer and may modulate autoimmune diseases in genetically susceptible individuals
Neurological conditions, especially Parkinson’s disease, have drawn growing attention as more research has emerged on environmental risk factors at Camp Lejeune. According to Neurology Live, Marines stationed at the base showed a higher risk of Parkinson’s disease, with volatile organic compounds (VOCs) and TCE identified as key contributors.
The 8 Presumptive Conditions vs. The 15 Covered Conditions
This distinction confuses many people — and for good reason. They serve different purposes within different VA programs.
According to the Department of Veterans Affairs’ official guidance on Camp Lejeune water contamination, here’s how they differ:
| Category | 8 Presumptive Conditions (Disability Compensation) | 15 Covered Conditions (Healthcare Benefits) |
|---|---|---|
| Purpose | VA disability compensation payments | VA healthcare with no copay for that condition |
| What “presumptive” means | VA automatically presumes your service caused the condition — you don’t need to prove causation | You’re covered for treatment of these conditions without copay |
| Conditions | Adult leukemia, Aplastic anemia/myelodysplastic syndromes, Bladder cancer, Kidney cancer, Liver cancer, Multiple myeloma, Non-Hodgkin’s lymphoma, Parkinson’s disease | All 8 above PLUS: Breast cancer, Esophageal cancer, Female infertility, Hepatic steatosis, Lung cancer, Miscarriage, Neurobehavioral effects, Renal toxicity, Scleroderma |
| Eligibility | 30+ days at Camp Lejeune/MCAS New River (Aug 1953–Dec 1987) + diagnosis | Same service requirement + diagnosis |
| Who qualifies | Veterans, Reservists, National Guard | Veterans AND eligible family members |
Note:“Presumptive“isn‘tthe same asautomatic. You‘ll still have to provide documentation military documents demonstrating you served at Camp Lejeune for the required period of time, and medical records establishing that you have the disease. The“Biblic“category simply means that you don‘thave to prove that you were exposedto the contamination causedyour illness not that you don‘t have to prove you were thereandthat you‘re sick.
Main Point: The evidence of association between the water and certain diseases at Camp Lejeune is genuine but a “limited / suggestive” body of evidence has not proven causation. There is a connection but not one you can establish based solely on population studies. You do not need to establish causation for the VA benefits presumptions to apply — the presumption establishes causation. However, the Justice Act established the statute that is an alternative to establishing causation for filing claims.
VA Benefits for Camp Lejeune Veterans and Families
Two separate VA benefit tracks exist for Camp Lejeune exposure. Understanding which applies to your situation is the first practical step.
Disability Compensation — The 8 Presumptive Conditions
If you were stationed at Camp Lejeune or MCAS New River for 30 cumulative days or more between August 1, 1953 and December 31, 1987, and were diagnosed with 1 of the 8 presumption illnesses, then you are eligible to apply for VA disability compensation.
The key advantage: you don’t need to prove your condition was caused by the contaminated water. The VA presumes the connection based on your qualifying service.
What you need to file:
- Military records indicating service on 30 or more cumulative days at Camp Lejeune, North Carolina, or MCAS New River, North Carolina, during the time period specified.
- Medical record evidence supporting the presence of one or more of the 8 presumptive conditions
- An established disability claim download application file using online at VA.gov, by taking it by mail, directly to a veterans regional office, or with the assistance of a veterans service organization (VSO)
What you do NOT need:
- A lawyer
- Proof that the water caused your condition
- A specific water test result or exposure record
Healthcare Benefits — The 15 Covered Conditions
In addition to disability compensation, eligible veterans who served at Camp Lejeune are eligible for VA health care. For any of the 15 covered conditions, you will not be charged a copay for treatment of that condition.
The 15 presumption covered conditions are all 8 presumption covered conditions as well as: Breast cancer, esophageal cancer, female infertility, hepatic steatosis, lung cancer, miscarriage, neurobehavoral effects, renal toxicity and scleroderma.
For many people, the first question is whether their current health problems might be related to the contaminated water. Common symptoms of contaminated water at Camp Lejeune include various cancers, neurological disorders such as Parkinson’s disease, and reproductive issues. This kind of symptom checklist can help you decide when to talk with your doctor and the VA about a possible connection.
Family Member Benefits
Applicable family members aka spouses, children (biological or adopted), or dependents were residents at Camp Lejeune and/or MCAS New River for 30 days or more during the qualifying period.
Supporting documentation to be submitted with a request to activate: VA Form 10-10068 and documentation showing eligibility: relationship to veteran, residence at Camp Lejeune during qualifying period(s), documentation of covered condition diagnosis.
In-utero exposure is considered. If you were in utero and your mother resided at Camp Lejeune any time during the qualifying period then you could qualify.
How to File a VA Claim (Step-by-Step)
- Collect your evidence-Gather your military service records that indicate your dates of Camp Lejeune assignment and medical records containing your diagnosis.
- Select your way to file Internet (va.gov), by mail, in person or VSO.
- Indicate Camp Lejeune When applying for benefits, say you are applying for one or more of the presumptive illnesses due to the Camp Lejeune water contamination
- Track and submit VA processes your claim, and you can track the status through VA.gov
- Think about VSO help Veterans Service Organizations will help you file claims at no cost. Don‘t pay anyone to do this.
The Camp Lejeune Justice Act of 2022 — Legal Claims Explained
Section 804 of the Honoring our Promise to Address Comprehensive Toxics (PACT) Act established an independent legal avenue (separate from VA benefits) for those injured by the water contamination at Camp Lejeune. This legal avenue is called the Camp Lejeune Justice Act of 2022.
It’s important to understand: this is a different track from VA benefits. You can pursue both simultaneously. But they work differently.
Who Can File Under the Justice Act?
You (or your legal representative) may file if:
- You lived, worked, or were otherwise exposed at Camp Lejeune for at least 30 cumulative days between August 1, 1953, and December 31, 1987, or
- Your mother met that requirement while pregnant with you
This is broader than VA disability eligibility — it includes civilian workers, contractors, and anyone who was on base, not just service members.
The Navy Elective Option vs. Filing a Lawsuit
Two paths exist under the Justice Act:
| Factor | Navy Elective Option | Federal Lawsuit |
|---|---|---|
| How it works | Administrative claim filed with the Department of the Navy for a faster settlement decision | Lawsuit filed in the U.S. District Court, Eastern District of North Carolina |
| Speed | Designed to be faster than litigation | Standard federal court timeline — potentially years |
| Who decides | Department of the Navy | Federal judge or jury |
| Offset rule | No offset — prior VA benefits do NOT reduce your settlement | Court must reduce award by the amount of any Camp Lejeune-related VA disability payments previously received |
| When to use | If you want a faster resolution without litigation risk | If the Navy denies your administrative claim, or you wait more than 6 months without a decision, or you prefer to pursue full litigation |
| Best when… | You want speed and certainty with no VA benefit offset risk | The Navy denies your claim, or you prefer full litigation with potential for a higher award |
One critical detail: accepting a settlement through the Navy’s elective option means resolving that claim administratively. If you choose this path, you’re accepting the Navy’s offer rather than pursuing the claim through federal court. Make sure you understand the terms before accepting.
You start by filing an administrative claim with the Department of the Navy. From there, you can either accept the Navy’s elective option for a faster settlement, or proceed to federal court if the claim is denied or unresolved after 6 months.
For information on filing, the Department of the Navy’s Camp Lejeune Justice Act claims portal provides official guidance and forms.
Will Filing a Claim Affect My VA Benefits?
Filing a Camp Lejeune Justice Act claim — whether administrative or lawsuit — will not affect your VA disability compensation or healthcare eligibility. Period.
However, there’s a nuance:
- If you pursue the Navy elective option and receive a settlement, that settlement does NOT reduce your VA benefits.
- If you file a federal lawsuit and a court awards you relief, the court is required to reduce (“offset”) that award by the amount of any VA disability payments or benefits you’ve already received that are related to Camp Lejeune water exposure specifically. VA benefits unrelated to Camp Lejeune are not affected.
This offset rule applies only to court judgments from lawsuits — not to the elective option settlements.
Worth noting: the Camp Lejeune Justice Act includes provisions designed to protect claimants from excessive legal fees. If you do choose to work with an attorney, be aware that fee structures in these cases are subject to federal oversight.
For questions about the claims process, you can contact the Department of Justice at 202-353-4426 or email camplejeune.pactact@usdoj.gov.
Common Mistakes and Misconceptions
Offered below are just a few of the common misconceptions you may have heard if you‘ve watched a Camp Lejeune commercial on the television. Thanks to both the flashy legal advertising campaigns and realities of two benefit systems working simultaneously, misinformation abounds. Here’s what actually holds up.
-
Myth: You need a lawyer to get VA benefits.
Reality: You do not need a lawyer for VA disability compensation or healthcare benefits. Veterans Service Organizations (VSOs) provide free claim assistance. The VA itself warns against commercials and firms claiming you can’t get benefits without their help. To report suspected fraud, call the VA at 800-488-8244.
-
Myth: “Presumptive” means your claim is automatically approved.
Reality: Presumptive designation eliminates the need to prove causation — not the need to prove you served at Camp Lejeune during the qualifying period and that you have a qualifying diagnosis. You still need documentation.
-
Myth: Filing a Camp Lejeune Justice Act claim will reduce your VA benefits.
Reality: Filing has no impact whatsoever on VA benefits. Only a court-awarded judgment (not the Navy‘s elective option settlement) can be offset, and only to the extent of the VA payments attributable to Camp Lejeune exposure.
-
Myth: Settlement amounts are predictable.
Reality: There is no credible, publicly available data on common settlement amounts as of early 2026 and averages. The dollar amounts discussed by anyone are the result of guesswork. The claims process is continuing to evolve and depends on the facts of each situation.
-
Myth: Everyone who was at Camp Lejeune will get cancer.
Reality: No disease occurs solely by exposure. The NIH/NRC review rated the evidence as “limited/suggestive,” that is, some associations have been observed but that does not mean it‘s a proven cause at the population level. Many factors influence individual risk, including dose, duration, and route, genetics, etc.
Who This Guide Is For — and Who Should Seek Specialist Help
This guide is for:
- Veterans who were stationed at Camp Lejeune or MCAS New River (1953 1987) and want to know about health risks and benefits will be able to access this information.
- Qualifying period to: spouses, children, and dependents who resided on base
- People exposed to in utero; whose mothers were residing at Camp Lejeune during pregnancy
- Anyone who is doing research, writing about, or championing an issue and needs a broad, unbiased, balanced, scholarly, and evidence-based overview.
This guide is NOT a substitute for:
- Personalized medical advice — if you have symptoms or a diagnosis, consult your healthcare provider
- Legal counsel for complex cases — if you’re deciding between the elective option and federal litigation, a qualified attorney experienced in Camp Lejeune claims can advise on your specific circumstances
- VA claims adjudication — this guide explains the process, but your individual claim will be evaluated based on your specific records
Final Verdict
The Ilene crisis is the most sustained(and one of the most significant) incidents of toxic exposure in American military history. For more than thirty years, service members and their families drank and bathed from water tainted by industrial chemicals. And despite years of investigation, the full picture — especially at Hadnot Point — is still incomplete.
What IS clear: federal law now provides two distinct pathways for affected individuals. VA benefits (disability compensation and healthcare) are accessible without a lawyer and carry no risk to existing benefits. The Camp Lejeune Justice Act of 2022 offers an additional legal pathway — through either the Navy’s elective option or federal court.
Practical recommendation: Start with VA benefits. They’re free to pursue, don’t require legal representation, and won’t be affected by any future legal claims. If you’re also considering a Justice Act claim, the elective option avoids the offset rule that applies to court judgments. Consult a VSO for claims assistance — their help is free.
The science is imperfect. It may never deliver the clear-cut answers people deserve. But the legal and benefit infrastructure is real, it’s accessible, and it’s available right now — and that’s worth acting on.
Frequently Asked Questions
Q: What diseases are linked to Camp Lejeune water contamination?
A: The VA lists 8 presumptive conditions for compensation (adult leukemia, kidney cancer, bladder cancer, liver cancer, multiple myeloma, Non-Hodgkin‘s lymphoma, aplastic anemia and Parkinson‘s disease) and for healthcare benefits (those listed for compensation, plus breast cancer, esophageal cancer, lung cancer, female infertility, hepatic steatosis, miscarriages, neurobehavioral effects, renal toxicity and scleroderma).
Q: How do I file a Camp Lejeune VA disability claim?
A: Gather your military service records showing 30+ days at Camp Lejeune or MCAS New River (August 1953–December 1987) and medical records confirming a presumptive condition diagnosis. File online at VA.gov, by mail, in person, or with a free Veterans Service Organization.
Q: Do I need a lawyer to get Camp Lejeune benefits?
A: No. VA disability and healthcare benefits do not require a lawyer. VSOs offer free assistance. The VA warns against TV commercials or firms claiming you can’t get benefits without paying for legal help.
Q: What is the Camp Lejeune Justice Act of 2022?
A: Camp Lejeune Justice Act. Title part of the PACT Act, it creates a mechanism for PACT Act claimants exposed to waters contaminated with solvents to obtain relief through either an administrative claim against the Navy (with an elective option for expedited settlement) or in a federal suit in the Eastern District of North Carolina.
Q: Will filing a Camp Lejeune lawsuit affect my VA benefits?
A: Filing will not affect your VA benefits. However, if a court awards you relief through a lawsuit (not via the Navy’s elective option), the award must be reduced by the amount of Camp Lejeune-related VA disability payments you’ve previously received.
Q: 8 Presumptive vs. 15 Covered Conditions
A: The 8 presumptive conditions qualify veterans for VA disability compensation payments — the VA presumes service connection without requiring proof of causation. The 15 covered conditions (which include all 8 plus seven more) qualify veterans and eligible family members for VA healthcare with no copay for those specific conditions.






")


")





")



